

Incidental Finding - Fourth Ventricular Tumor Requiring Immediate Removal
/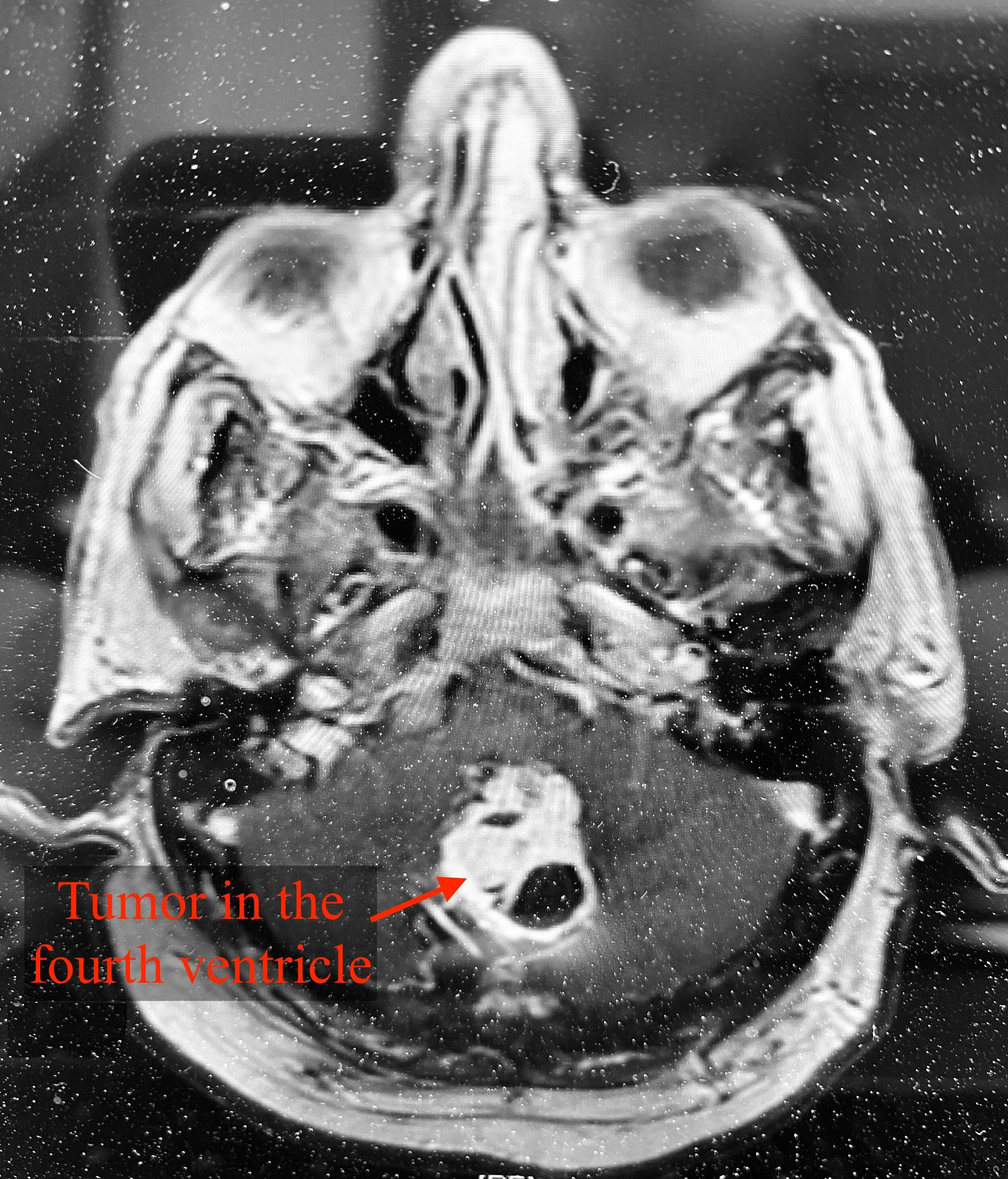
Tumor (Preoperative)
DT, a middle aged man, had been experiencing worsening balance over the past few weeks. One morning he became so unsteady that he fell while traversing a doorway and hit his head. He sustained a severe injury to his face, prompting a visit to the emergency department.
In the ER, DT spoke with his physician about his difficulty balancing, which led to his fall, injury, and resulting facial pain and headaches. After preliminary assessments and discussion of possible fainting, DT was sent to get a head CT.
As suspected, the CT revealed a nasal bone fracture. However, incidentally, the head CT also showed a left cerebellar hemisphere mass in the posterior fossa, which was likely causing obstructive hydrocephalus. This meant the flow of his cerebral spinal fluid was being blocked at his fourth ventricle.
His treatment team then followed up with an MRI, which helped determine that the mass was likely a tumor originating from his cerebellum. It also showed that the tumor was causing severe obstructive hydrocephalus and mass effect. Thankfully it was unlikely to be cancerous; however, its removal was necessary due to the significant symptoms it was causing. His loss of stability was worsening and he was developing other balance issues, like truncal ataxia, dysmetria, and nystagmus. It was determined that this tumor was the probable cause of his current injury and could not be left untreated. He needed immediate surgical intervention to prevent the complete blockage of his fourth ventricle.
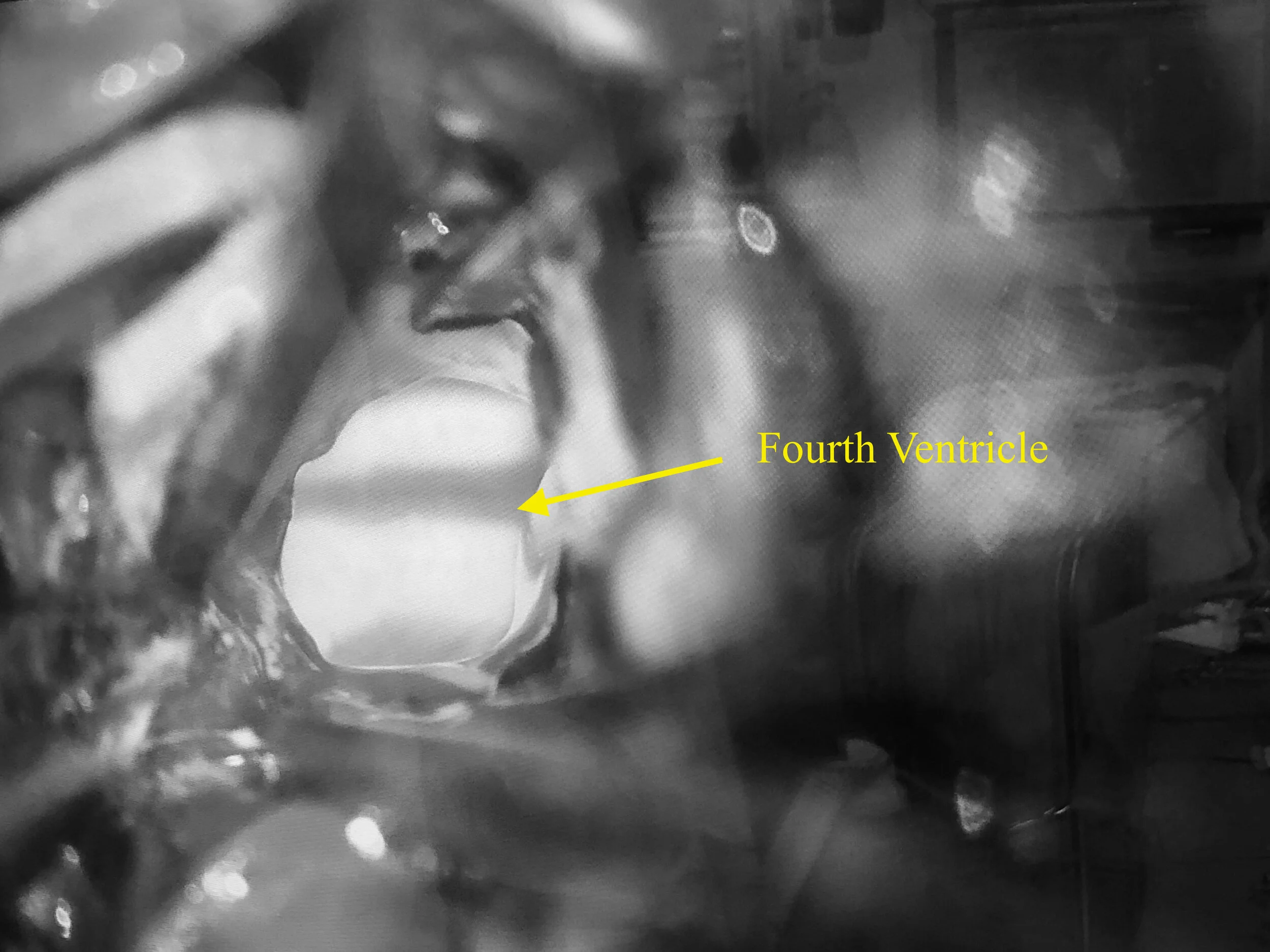
Intraoperative microscopic view
Unfortunately DT was unemployed and uninsured. He would not be able to afford the necessary surgery, so INI jumped into action! We secured his operative team, which included a pair of neurosurgeons for his exceptionally intricate case, ensuring everything would be at no cost to DT.
The following day, DT went under anesthesia and the suboccipital craniectomy began. Under extremely high magnification, microsurgical dissection was conducted on the severely adherent tumor. The tumor was found to be too vascular for ultrasonic aspiration, therefore only bipolars and microdissection instruments could be used for the image guided brain tumor resection. After 12 meticulous hours in the OR, almost all of the tumor was able to be removed. Resections of the tumor were sent to pathology, where they were all diagnosed as hemangioblastoma, which is a benign, vascular brain tumor.
DT tolerated the surgery well and is now recovering in the ICU.

(Left to right) Dr. Vokshoor, DT, and Dr. Ament
